Line 1. The mood dysregulation of the personality disorder patient is manifested by
"positive'' symptoms such as lability, rejection sensitivity,
inappropriate intense anger, depressive "mood crashes,'' and
temper outbursts. These are most characteristic of Cluster B patients.
"Negative mood states,'' including anhedonia and a "cold,
constricted affect,'' are more prevalent among the schizoid, paranoid,
and schizotypal patients of Cluster A. Excessive anxiety, as an
affective state, is ubiquitous across categories, though perhaps most
commonly associated with Cluster C patients. Dysregulation or
disinhibition of affect may have a basis in serotonergic function
quite separate from the specific affect expressed, whether anger,
depression, or anxiety. It is important to recognize the context in
which affective dysregulation occurs. Anger, in the context of
cognitive-perceptual symptoms in a Cluster A patient, responds well to
dopamine blockade, that is, low-dose neuroleptics. In the context of
reactive depressive moods, as in the temper tantrums of a Cluster B
patient, enhancing serotonergic function may be the preferred mode of
treatment (i.e., SSRI antidepressants).
Line 2. The psychobiology of affective dysregulation may involve
disinhibition of emotional expression through diminished central
actions of serotonin in the prefrontal cortex. Personality disorder patients presenting
with syndromes of affective disinhibition. whether depressed, angry.
or anxious. should be treated initially with one of the SSRI
antidepressants. Research support for the efficacy of SSRI
antidepressants against the depressive moods and dysregulated anger of
PD patients has been demonstrated in two double-blind, randomized,
placebo-controlled studies (Markovitz, 1995; Salzman et al., 1995) and
four open label case series (Cornelius et al., 1990; Kavoussi et al.
1994; Markovitz et al., 19919 Norden, 1989), thus warranting an
"A'' level of support. SSRI antidepressants have the additional
advantages of a broad spectrum of therapeutic effects, relative safety
in overdose (e.g.. compared to the tricyclic or MAOI antidepressants),
and favorable side-effect profiles, supporting compliance. Fluoxetine
has been found useful against depressed mood. lability, rejection
sensitivity, impulsive behavior, self-mutilation, hostility, and even
psychoticism. Research trials have ranged in duration from 6 to 14
weeks for acute treatment studies, with continuation studies up to 12
months. Individual patients have retained improvement on maintenance
treatment from 1 to 3 years. Studies have been reported with
fluoxetine, in doses of 20-80 mg/day and sertraline, in doses of
100-200 mg/day or 200-600 mg/day (Markovitz, 1995). A fair treatment
trial of SSRI antidepressants is 4-6 weeks.
Research experience with tricyclic antidepressants (TCAs) in PD
patients has produced inconclusive results. Although patients with
comorbid major depression and PD improve with TCAS, the effects of
both TCA and MAOI antidepressants in patients with primary diagnoses
of BPD have been demonstrated to be independent of Axis I diagnoses of
comorbid depression (Cowdry & Gardner, 1988; Soloff, George,
Nathan, Schulz, Ulrich, & Perel, 1986b). In one placebo-controlled
study, amitriptyline was associated with a paradoxical behavioral
toxicity in patients with BPD, increasing suicidal ideation, paranoid
thinking, and assaultiveness significantly more than among placebo
nonresponders (Soloff, George, Nathan, Schulz, & Perel. 1986a).
Line 3. In studies of Axis I affective disorders, acute treatment
is usually 6-12 weeks, continuation is 4-9 months, and maintenance is
longer than 1 year. Since affective dysregulation is a dimension of
temperament in the PD patient, and not an acute illness, the duration
of continuation and maintenance phases of pharmacotherapy cannot
presently be defined. Significant improvement in the quality of the
patient's coping skills and interpersonal relationships may be
required before medication support can be discontinued.
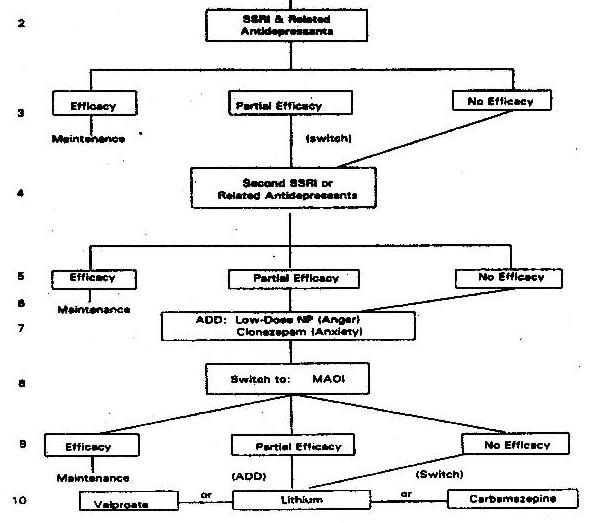
Line 4. In the event of a suboptimal response, the patient should
be switched to a second SSRI or related antidepressant (i.e., the
so-called "salvage'' strategy). Depressed patients who fail to
respond to one SSRI antidepressant may still respond to a second
member of the same family. In a study of borderline patients, half of
patients who failed to respond to fluoxetine responded to a trial of
sertraline (Markovitz, 199.5). Given the paucity of research on the
question of "salvage'' strategies with SSRI antidepressants in
personality disorder patients, this decision is supported only at the
"C'' level. Among the SSRl-related antidepressants, only
venlafaxine has been studied in patients with a primary diagnosis of
PD in one open label trial (Markovitz & Wagner, 1995). Efficacy
was demonstrated against somatic complaints, which were prominent in
this sample, with robust effect sizes on overall global improvement.
Lines 5, 6. As noted earlier, there are no empirical guidelines for
continuation or maintenance therapy when the target symptom is part of
temperament. Clinical experience suggests caution in discontinuing a
successful medication trial of antidepressants against affective
dysregulation when the patient has failed multiple prior medication
trials.
Line 7. When significant anxiety accompanies the clinical
presentation, the SSRI antidepressant may be insufficient, or, at
least, untimely. At this point, some consideration should be given to
the use of benzodiazepines. Anxiety in the PD patient may present as a
chronic and nonspecific complaint, the "pan-anxiety'' of older
description, or as an exaggerated response to a social stressor. The
use of benzodiazepines is problematic in the treatment of patients
with PD, raising the risk of abuse and even behavioral toxicity. The
short-acting benzodiazepine alprazolam has been associated with
precipitating serious dyscontrol in one placebo-controlled crossover
study of patients with BPD (Gardner & Cowdry, 1985). Abuse
potential is significant and tolerance problematic over time. Case
reports demonstrate some efficacy in the PD patient for the long
half-life benzodiazepine clonazepam, which has anticonvulsant and
antigenic properties (Faltus, 1984; Freinhar & Alvarez, 1986).
Clonazepam has very high affinity for the benzodiazepine receptor and
may be used in low doses. It has been shown to increase serotonin
synthesis and function in humans, and unregulated the density of
serotonin receptor sites in animals (Chouinard, 1987). These
serotonin-enhancing properties may be involved in the efficacy of
clonazepam against agitation and increased motor activity in manic
patients and in its beneficial effects on anxiety and impassivity,
including violent outbursts, in the PD patient. Clonazepam is best
used adjunctively with the SSRI antidepressants. As research is
generally lacking on the use of benzodiazepines in the Personality
Disorder patient,
support for these recommendations is at the "C'' level.
Buspirone may offer some prophylactic benefit against vulnerability
to anxiety without the risk of abuse or tolerance; however, the
absence of an acute effect generally makes this drug less acceptable
to PD patients. Buspirone may confer some benefit against impulsive
aggression or enhance the efficacy of SSRI antidepressants through
synergistic effects on the serotonin system. At present, there is
insufficient published experience with buspirone in the PD patient to
permit inclusion in a clinical algorithm.
Where anger is the predominant affect, yet coexists within an
otherwise affective presentation, SSRI trials are still preferred as
the treatment of first choice. Salzman et al. (1995) have demonstrated
the efficacy of fluoxetine against anger in the Borderline Personality
Disosrder patient
independent of effects on depressed mood. Effects of fluoxetine on
anger and impulsivity may appear within days, much earlier than
antidepressant effects. However, if the patient presents in poor
behavioral control, if risk of dyscontrol is high and time is of the
essence, low-dose neuroleptics can be added to the regimen for rapid
response. Low-dose neuroleptics confer the additional benefit of
diminishing the severity of affective symptoms. Augmentation with
neuroleptics should be considered before moving to the use of MAOI
antidepressants, which require more patient cooperation and
compliance.
Line 8. MAOI antidepressants follow SSRI and related
antidepressants primarily because of concerns for safety, compliance
with diet, and a less favorable side-effect profile. Clinicians who
wish to use MAOI antidepressants as the second line of treatment
should use the short half-life SSRI antidepressants first, for
example, sertraline or paroxetine, avoiding the 35-day washout
required for fluoxetine, before starting the MAOI (i.e., 2-week
washout of sertraline or paroxetine should be sufficient). As a class,
MAOI antidepressants have support for efficacy in personality
disorders from two placebo-controlled studies in which borderline
personality disorder was a
primary diagnosis (Cowdry & Gardner, 19889 Soloff et al., 1993)
and in studies of closely related diagnoses, that is, "hysteroid
dysphoria'' and ''atypical depression,'' in which the diagnosis of
personality disorder was considered secondary (Parsons et al., 1989).
The study of Cowdry and Gardner (1988) demonstrated significant
effects against behavioral impulsively, mood reactivity, and rejection
sensitivity, while the Cornelius et al. (1993) study showed an effect
against anger and hostility. Effects against atypical depression or
"hysteroid dysphoria'' are reported in studies where the PD was
secondary to the primary "atypical'' affective disorder (Parsons
et al. 1989). A "B'' level of support seems most appropriate for
this recommendation.
Lines 9, 10. If an MAOI antidepressant has demonstrated no efficacy
against lability. a mood stabilizer should replace the MAOI
antidepressant. If partial efficacy has been achieved with the MAOI
antidepressant, the mood stabilizer may be used as an augmenting
agent. Lithium carbonate, carbamazepine, and valproate are useful in
the treatment of labile mood in the context of Axis I bipolar
disorders and have been used empirically against the mood instability
of Axis 11 patients. Among the three mood stabilizers, lithium
carbonate has the most research support in double-blind,
placebo-controlled studies with PD patients, although these studies
have focused on impulsive aggression rather than on mood regulation
and are reviewed in the next section. An early study of female
adolescents diagnosed as having "emotionally unstable character
disorder'' (EUCD), reported specific improvements in lability of mood
with lithium treatment (Rifkin, Levitan, Galewski, & Klein, 1972).
The diagnostic validity of EUCD has not withstood the test of time,
resulting in the diagnosis being deleted in DSM-III. A recent
double-blind, placebo-controlled study comparing lithium to
desipramine and placebo against depressed mood in borderline patients
found no significant differences between the three against depressive
symptoms, although more patients on lithium (vs. placebo) tended to
have improvements in anger, suicidal symptoms, and impulse control.
Global assessments by therapists favored the lithium-treated patients
because of its effects on impulse control (Links, 1990). Lithium
carbon- ate has the disadvantages of a narrow margin of safety in
overdose, the risk of hypothyroidism in chronic use, and the need for
monitoring blood levels. Because of the close association between
disinhibition of mood and impulse, lithium is the preferred choice for
affective lability among the three mood stabilizers; however, support
for efficacy specifically against affective dysregulation is
admittedly low (Level C).
Carbamazepine has demonstrated efficacy against behavioral
impulsivity, anger, suicidality, and anxiety in the context of BPD
patients with "hysteroid dysphoria'' in one double-blind,
placebo-controlled cross-over study (Cowdry & Gardner, 19879
Gardner & Cowdry, 19#6b). However, a recent, well-controlled study
of BPD patients with no Axis I affective disorder found no significant
benefit to carbamazepine as compared to placebo (De La Fuenta &
Lotstra, 1994). As to behavioral toxicity. carbamazepine has
precipitated melancholic depression in borderline patients with a
history of this disorder (Gardner & Cowdry, 1986a). Medical
precautions associated with the use of carbamazepine include the risk
of bone marrow suppression and the need to follow hematologic
parameters as well as blood levels of the drug.
Valproate has demonstrated some efficacy in open label
case studies of patients with BPD and may have some utility against
agitation, aggression, and anxiety among severely disturbed inpatients
(e.g.. less time in seclusion) (Wilcox, 1995). Among outpatients with
BPD, valproate is associated with modest overall improvement in mood,
anxiety, anger, impassivity, rejection sensitivity, irritability, and
overall symptom severity in half of patients studied (Stein, Simeon,
Frenkel, Islan, & Hollander, 1995). At this time, there is a
paucity of research data on the use of carbamazepine and valproate in
the PD patient, warranting a "C'' recommendation.