Soloff, Algorithm 3Algorithm for treatment of impulsive-behavioral symptoms
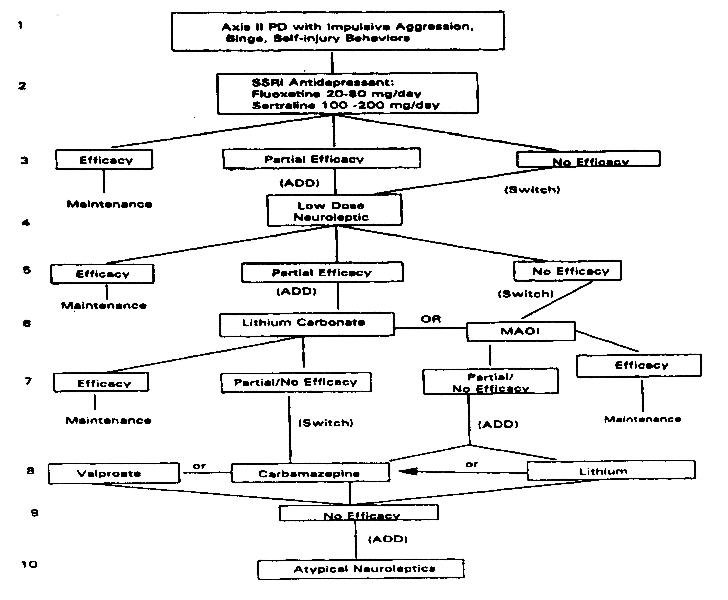 Figure 3
Figure 3
Line 1. The algorithm for the treatment of impulsive-behavioral symptoms in the PD patient bears a strong resemblance to that for affective dysregulation, as they share some elements of a common pathophysiology. The impulsive-behavioral symptoms of the PD patient are the endpoint of a process of disinhibition of affect, impulse, and cognition. Although most dramatically expressed in self-destructive or assaultive acts, impulsivity can be manifested in a broad spectrum of symptomatic behaviors (e.g., binges of eating, spending. sex, drugs) or as cognitive impassivity (e.g., rash judgments).
Impulsive-aggressive behavior in patients with personality disorders, including suicide, homicide, and other violent behaviors, correlates with diminished levels of cerebrospinal fluid (CSF) 5-HIAA and blunted neuroendocrine responses to serotonergic pharmacodynamic challenges (e.g., with d,l-fenfluramine, m-cholorophenylpiperazine, and buspirone) independent of affective disorder (Coccaro et al., 1989; Mann, Arango, Marzyk, Theccanat, & Reis, 19899 Siever & Trestman, 1993). Diminished levels of CSF 5-HIAA may represent a marker for vulnerability to suicidal behavior, particularly attempts by violent means. Diminished CSF 5-HIAA is also found in personality disorder patients who have committed impulsive violent crimes, including homicide. It is reported in patients who have killed their children or persons emotionally close to them, as opposed to strangers (Lidberg, Tuck, Asberg, Scalia-Tomba, & Bertisson, 1985; Linnoila et al., 1983). Diminished levels of CSF 5-HIAA have been found in borderline patients years after serious suicide attempts, suggesting that diminished serotonergic neurotransmission is a marker for suicidal behavior in this population (Gardner, Lucas, & Cowdry, 1990). Diminished central serotonergic function has also been demonstrated in Type II alcoholics who are males with early onset drinking and antisocial personalities (Limson et al., 1991). Current theory holds that the executive functions of response inhibition are mediated in prefrontal cortex by serotonergic neurotransmitter function (Weinberger, 1993). Recent studies of impulsive-aggressive individuals using positron emission tomography (PET) neuroimaging techniques demonstrate decreased activation in prefrontal cortex consistent with clinical symptoms of disinhibition (Rain: et al.,1992).
Line 2. The SSRI antidepressants are the treatment of first choice for impulsive, disinherited behavior in the context of PD. The effect of SSRI antidepressants on impulsive behavior is independent of the effect on depression and is supported by two placebo-controlled studies and five open label trials, utilizing fluoxetine and sertraline, warranting a support level of "A'' (Coccaro et al., 1990; Cornelius et al., 1990; Kavoussi et al., 1994; Markovitz, 1995; Markovitz et al., 1991; Norden, 1989; Salzman et al., 199.5).
Line 3. The effects of SSRI antidepressants on impassivity appear earlier than the effects on depression, with onset of action within days in some reports. Similarly, discontinuation of drug following successful treatment results in the reemergence of impulsive aggression within days. The duration of treatment following successful management of impulsive aggression is determined by the clinical state of the patient, including risk of exposure to life stressors and progress in learning coping skills. When the target for treatment is a trait vulnerability, one cannot set a predefined limit on treatment duration. Line 4. In the event of partial efficacy, or where clinical need is urgent, a low-dose narcoleptic may be added. Double-blind trials with BPD patients have demonstrated anti-impulse actions of low-dose neuroleptics. The effect of neuroleptics in the PD patient may be nonspecific, diminishing symptom severity across a broad spectrum of symptoms. Nonetheless, the effect is rapid in onset, often in hours with oral use (more rapidly intramuscularly, if needed), and may provide urgent control over escalating impulsive aggression. Low-dose neuroleptics can be started before the full fair trial of SSRI antidepressant is complete. In the event of no efficacy to the SSRI antidepressant, and where time permits, a "salvage'' trial of a second SSRI or related antidepressant may be considered, although there are no published clinical trials of second SSRIs with impassivity as a target symptom.
Lines 5, 6. Partial efficacy to an SSRI antidepressant may be enhanced through addition of lithium carbonate for its proven anti-impulse effects. Studies by Tupin et at., (1973) of impulsive, criminal adults and by Sheard (1975) of delinquent adolescents demonstrate a strong effect for lithium carbonate against the impulsive-aggressive symptoms of the PD patient. The double-blind studies and additional case reports (e.g., Shader, Jackson, & Dodes, 1974) support an "A'' recommendation for the use of lithium for this indication.
In the event of no response to the SSRI trials, MAOI antidepressants are recommended. Cowdry and Gardner (1988) demonstrated efficacy against behavioral impassivity for tranylcypromine in a placebo-controlled crossover study of women with BPD and "hysteroid dysphoria.'' Soloff et al.,(1989) found phenelzine effective against anger and irritability in BPD patients, although not against other affective complaints. As both of these studies were double blind and placebo controlled, the MAOI recommendation for use in impulsively, anger, and irritability is supported at the "A'' level. Combining an MAOI antidepressant with lithium or an anticonvulsant as augmentation would also appear to be rational treatment at this point, although there are no studies of these combinations.
Lines 7, 8. The use of carbamazepine or valproate for impulse control in the PD patient appears to be widespread in clinical practice (based on their efficacy in bipolar disorders), although research studies are inconclusive for efficacy against impulsive aggression. Cowdry and Gardner (1988; Gardner & Cowdry, 1986b) reported efficacy for carbamazepine against behavioral impulsively in the context of borderline disorder with comorbid "hysteroid dysphoria.'' However, a recent report by De La Fuenta et al., (1994) failed to replicate this finding in a well-controlled study that excluded patients with affective disorders. Pending further research, the level of support for carbamazepine for the specific indication of impulsive aggression in the PD patient remains at the "C'' level.
Support for the use of valproate as a treatment for impulsively in the PD patient is derived from case reports and one open label trial in which impulsively was significantly diminished among severely impaired borderline patients (Stein et al., 1995; Wilcox, 1995). Valproate has also been shown to be helpful against the chronic temper outbursts and mood lability of adolescents with "disruptive'' behavior disorders (e.g., ADHD. oppositional disorder, conduct disorder) (Donovan et al., 1997). The paucity of controlled studies requires a "C'' level of support for this indication for valproate.
Lines 9, 10. Finally, the atypical neuroleptics may have some efficacy in the treatment of impulsively, especially against severe self-mutilation or other impulsive behaviors arising from psychotic thinking in the context of BPD. Support is at the "C'' level, derived from one open label trial and one case report (Chengappa et al., 19959 Frankenburg & Zanarini, 1993). The difficulties and risks involved in using clozapine (e.g., neutropenia) warrant its place as treatment of last resort. The newer atypical neuroleptics do not cause neutropenia and warrant further exploration in the treatment of patients with refractory impulsive aggression.
Novel approaches
Novel approaches merit consideration by clinicians faced with specific refractory symptom presentations, although the lack of clinical testing or widespread experience prohibits recommendation in a general clinical algorithm.
Opiate antagonists
The repetitive self-injurious behavior (SIB) of the patient with BPD has been treated with the opiate antagonist naltrexone following the hypothesis that endogenous opiates may be involved in the initiation or maintenance of self-injury. Evidence suggesting a role for the opiate system in SIB includes reports of increased plasma metenkephalin in habitual mutilators, increased pain thresholds in BPD patients with histories of SIB, and the phenomenon of topical analgesia in SIB, which can be blocked by opiate antagonists (Russ, R0th, Kakuma, Harrison, & Hull, 1994). Treatment trials in mentally retarded subjects suggest modest results against SlB. Case reports and small patient series support a similar role in patients with BPD (McGee, 1997; Sonne, Rubey, Brady, Malcolm, & Morris, 1996).
Psycbostimulants
Is there a role for the Psycbostimulants in treating personality disorders? Impulsivity often presents as a residual adult symptom of childhood attention-deficit/hyperactivity disorder (ADHD). It is not always possible to clearly distinguish the impulsive temperament of the antisocial or borderline patient from the residual impassivity of the adult with ADHD. The two syndromes may even be comorbid in some cases. Where a clearly defined childhood syndrome of ADHD precedes development of adult personality disorder, use of a psychostimulant as treatment for adult impulsively is more appropriately viewed as maintenance treatment for the residual symptoms of an Axis I disorder. Given the abuse potential of the Psycbostimulants, full exploration of antidepressant efficacy, including buproprion (which has dopaminergic actions and is useful in ADHD), should precede any trial of psychostimulants in the PD patient. Psychostimulants may also be helpful as activating agents in the treatment of severely anergic, amotivational depressive states, although they are not truly antidepressant in this usage. The careful use of these agents in the PD patient for anergic depressed mood has some clinical utility, although there is no research support for the practice at the present time.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual oriental disorders (4th ed.). Washington, DC: Author.
Chengappa, K. N., Baker, R. W., & Sirri. C. (1995). The successful use of clozapine in ameliorating severe self-mutilation in a patient with borderline personality disorder. Journal of Personality Disorders, 9, 76-82.
Chouinard, G. (1987). Clonazepam in acute and maintenance treatment of bipolar affective disorder. Journal of Clinical Psychiatry. 4#(10. Suppl.), 29-36.
Cloninger, C. R., Svrakic, D. M., & Przybeck, T. R. (1993). A psychobiological model of temperament and character. Archives of General Psychiatry, 50, 975-990.
Coccaro, E. F., Astill, J. L., Herbert, J. L., & scout, A. G. (1990). Fluoxetine treatment of impulsive aggression in DSM-III-R personality disorder patients. Journal of Clinical Psycbopharmacology. 105, 373-375.
Coccaro, E. F.. Siever, L. J., Klar, H. M., Maurer, G., Cochrane, K., Cooper, T. B.. Mobs. R. C., & Davis, K. L. (1989). Serotonergic studies in patients with affective and personality disorders: Correlates with suicidal and impulsive aggressive behavior. Archives of General Psychiatry. 46, 587-599.
Cornelius, J. R., Soloff, P. H., Peres, J. M., & Ulrich, R. ( 1990). Fluoxetine trial in borderline personality disorder. Psychopharmacology Bulletin. 26, 149-152.
Cornelius, J. R., Soloff, P. H., Perel, J. M.. & Ulrich, R. F. (1993). Continuation pharmacotherapy of borderline personality disorder with Haloperidol and Phenelzine. American Journal of Psychiatry. 15% 1843-1848.
Costa, P. T., Jr., & Mccrae, R. R. (1992). Normal personality assessment in clinical practice: The NEO personality inventory. Psychological Assessment.4. 5-13.
Cowdry, R. W., & Gardner, D. L. (1988). Pharmacotherapy of borderline personality disorder: Alprazolam. Carbamazepine, Trifluoperazine and Tranylcypromine. Archives of General Psychiatry. 45. 111-119.
De La Fuenta, J. M., & Lotstra. F. (1994). A trial of Carbamazepine in borderline personality disorder. European Neuropsychopharmacology. 4. 479-486.
Donovan, S. J., Susser, E. S., Nynes. E. V., Stewart, J. W.. Quitkin. F. M., & Klein, D. F. (1997). Divalproex treatment of disruptive adolescents: A report of 10 cases. Journal of Clinical Psychiatry, 58, 12-18.
Eysenck, H. J., & Eysenck. S. B. ( 1976). Manual of the EPQ (Eysenck personality Questionnaire). San Diego, CA: Educational and Industrial Testing service.
Faltus, F. ( 1984). The positive effect of Alprazolam in the treatment of three patients with borderline personality disorder. American Journal of Psychiatry. 141 , 802-803.
Frankenburg, F. R., & Zanarini, M. C. (1993). Clozapine treatment of borderline patients: A preliminary study. Comprehensive Psychiatry. 34. 402-405.
Freinhar, J. P., & Alvarez, W. A. (1986). Clonazepam: A novel therapeutic adjunct. International Journal of psychiatry in Medicine, 15(4). 32 1-328.
Gardner, D. L., & Cowdry, R. W. (1985). Alprazolam-induced dyscontrol in borderline personality disorder. American Journal of Psychiatry, 142. 98-100.
Gardner, D. L., & Cowdry, R. W. (1986a). Development of melancholia during Carbamazepine treatment in borderline personality disorder. Journal of Clinical Psycopharamcology, 6, 236-239.
Gardner. D. L., & Cowdry R. W. ( 19#6b). Positive effects of Carbamazepine on behavioral dyscontrol in borderline personality disorder. American Journal of Psychiatry. 143, 519-522.
Gardner, D. L., Lucass P. B., & Cowdry, R. W. (1990). CSF metabolites in borderline personality disorder compared with normal controls. Biological Psychiatry. 28. 247-254.
Goldberg. S. C., Schulz, S. C., Schulz, P. M.. Resnick, R. J., Hamer, R. M., & Friedel. R. 0. (19863. Borderline and schizotypal personality disorders treated with low-dose Thiothixene vs. placebo. Archives of General Psychiatry. 43, 680-686.
Jobson, K. 0., & Potter, W. Z. (199.5). International psycopharmacology algorithm project report. Psychopharmacology Bulletin. 31(3). 457-507.
Kavoussi, R. J., Liu, J., & Coccaro, E. F. (1994). An open trial of serialize in personality disordered patients with impulsive aggression. Journal of Clinical Psychiatry, 55(4), 137-141.
Kelly, T., Soloff, P. H.. Cornelius. J. R.. George, A.. & Lis. J. (1992). Can we study (treat) borderline patients? Attrition from research and open treatment. Journal of Personality Disorders, 6, 417-433.
Kutcber, S.. Papatheodorou, G., Reiter, S., & Gardner, D. (1995). The successful pharmacological treatment of adolescents and young adults with borderline personality disorder: A preliminary open trial of Flupenthixol. Journal of Psychiatry and Neuroscience. 20(21, 113-1 18.
Lidberg, L., Tuck, J. R., Asberg, M.. Scalia-Tomba, G., & Bertisson, L. ( 1985). Homicide, suicide and CSF S-HIAA. Acta Psycbiatrica Scandinavica, 71. 230-236.
Limson, R., Goldman, D., Roy, A., Lemparski, 0., Ravitz, B., Adinoff, B., & Linnoila, M. (1991). Personality and cerebrospinal fluid monoamine metabolites in alcoholics and controls. Archives of General Psychiatry, 48, 437-441.
Links, P. (1990). Lithium therapy for borderline patients. Journal of Personality Disorders, 4, 173-181.
Linnoila, A., Virkkunen, M., Scheinin. M., Nuutila. A., Rimon. R.. & Goodwin, F. K.(1983). Low cerebrospinal fluid ws-hydroxy-indol: acetic acid concentrations differentiate impulsive from non-impulsive violent heavier. Life Sciences. 33. 2609-2614.
Mann, J. J., Arango, V., Marzyk, D. M., Theccanat, S., & Rein, D. J. ( 1989). Evidence for the S-HT hypothesis of suicide: A review of postmortem studies. British Journal of Psychiatry, 1.5-.5'48), 7-14.
Markovitz, P. J. (19951. Pharmacotherapy of impassivity, aggression and related disorders. In E. Hollander & D. Stein (Eds.), Impassivity and aggression (pp. 263-287). Surrey, United Kingdom; Wiley.
Markovitz, P. J., Calaboose, J. R., Schulz, S. C., & Meltzer, H. Y. ( 1991). Fluoxetine in the treatment of borderline and schizotypal personality disorders. American Journal of Psychiatry 148. 1064-1067.
Markovitz, P. J., & Wagner, S. L. ( 1995). Venlafaxine in the treatment of borderline personality disorder. Psychopharmacology Bulletin. 31(4), 773-777.
McGee, M. D (1997). Cessation of self-mutilation in a patient with borderline personality disorder treated with Naltrexone (Letter to the editors. Journal of Clinical Psychiatry .58(1), 32-33.
Montgomery, S. A., & Montgomery, D. ( 1982). Pharmacological prevention of suicidal behavior. Journal of Affective Disorders, 4, 291-298.
Norden, M. J. ( 1989). Fluoxetine in borderline personality disorder. Progress in Neuropsychcopharmacology and Biological Psychiatry. 13, 885-893.
Parsons, B., Quitkin, F. M.. McGrath, P.J., Stewart. J.W., Trilam, 0. E., Ocepek-welikson, K., Harrison, W., Rabkin. J. G.. Wager. S. G.. & dynes. E. ( 1989). Phenelzine, Imipramine and placebo in borderline patients meeting criteria for atypical depression. Psychopharmacology Bulletin, 25, 524-534.
Raine, A.. Bpchsbaum, M. S., Stanley, J., Lottenberg. S.. Abel, L., & Stoddard, J. (1992). Selective reductions in prefrontal glucose metabolism in murderers assessed with positron emission tomography. Psychophysiology. 29(4A). 558.
Rush. A.J.. Prio, R. F. (1995). From scientific knowledge to the clinical practice of Psychopharmacology: Can the gap be bridged? Psychopharmacology Bulletin, 31, 7-20. '
Rifkin, A.. Levitan, S. J., Galewski, J., & Klein, D. F. (1972). Emotionally unstable character disorder: A follow-up study. Biological Psychiatry, 4, 65-79.
Russ. M. J., Roth, S. D., Kakuma, T., Harrison, K., & Hull, J. W. ( 1994). Pain perception in self-injurious borderline patients: Naloxone effects. Biological Psychiatry, 35. 207-209.
Jazzman, C., Wolfson, A.N., Scharzberg, A., Looper, J., Henke, R., Albanese, M., Schwartz, J., & Miyawaki, E. (199.5). Effect of Fluoxerine on anger in symptomatic volunteers with borderline personality disorder. Journal of Clinical Psychopharmacology, 15, 23-29.
Shader, R.I., Jackson, A.H., & Dodes, L. M. ( 1974). The anti-aggressive effects of lithium in man. Psycbopbarmacologia (Berlin), 40, 17-24.
Shears. M. H. (1975). Lithium in the treatment of aggression.. Journal of Nervous and Mental Diseases 160, 108-113.
Siever, L. j., & Trestman, R. ( 1993). Multifactorial models of neurotransmitter mediated disorders. International Clinical Psychopharmacology, 8, 33-39.
Soloff, P. H., Cornelius. J., George, A., Nathan. S.. Peres. J. M.. & Ulrich, R. F. (1993). Efficacy of Phenelzine and Haloperidol in borderline personality disorder. Archives of General Psychiatry, 50, 377-385.
Soloff, P. H., George, A., Nathan, R. 5., Schulz, P. M., Cornelius, J. R.. Herring, J., & Perel, J. M. (1989). Amitriptyline vs. Haloperidol in borderlines: Final outcomes and predictors of response. Journal of Clinical Psychopharmacology, 9(4), 238-24#.
Soloff, P. H.. George, A., Nathan, R. S., Schulz, P. M., & Perel, J. M. (1936a). Paradoxical effects of Amitriptyline in borderline patients. American Journal of Psychiatry, 143, 1603-1605.
Soloff, P. H., George, A., Nathan, S., Schulz, P. M., Ulrich, R. F.. & Perel, J. M. (19#6b). Progress in pharmacotherapy of borderline disorders. Archives of General Psychiatry, .3, 691-697.
Sonne, S., Rubey, R.. Brady, K., Malcolm, R., & Morris, T. ( 1996). Naltrexone treatment of self-injurious thoughts and behaviors Journal of Nervous and Mental Disease, 184(3), 192-195.
Stein, D. J., Simeon, D., Frenkel, M., Islan, M. N.. & Hollander, E. (1995). An open trial of Valproate in borderline personality disorder. Journal of Clinical Psychiatry. 56. 506-510.
Tupin. J. P., Smith, D. B., Claxon, T. L., Kim, L. 1., Nugent, A., & Groupe, A. (1973). Long-term use of lithium in aggressive disorders. Comprehensive Psychiatry, 14, 31 1-317.
Weinberger, D. R. (1993). A contortionist approach to the prefrontal cortex. Journal of Neuropsychiatry and Clinical Neuroscience, 5, 241-2.53.
Wilcox, J. A. (1995). Divalproex sodium as a treatment for borderline personality disorder. Annals of Clinical Psychiatry 7(1). 33-37.
Contributed by Valerie Porr, President of TARA APD